Climate change and health: what you need to know
A guide for public health professionals, health communicators, and anyone who wants to understand why the climate crisis is a health crisis
Person holding 'There is No Planet B' poster in San Francisco, United States © Li-An Lim/Unsplash
Climate change and health are not two conversations. They are one, and the longer we treat them as separate, the more people pay for that mistake with their health.
I’ve been an environmentalist for as long as I can remember, but volunteering with the Haribon Foundation in 2014 and being a member since made me more intentional about advocating for a sustainable environment and protecting biodiversity. Even then, I thought of it as separate from my day job in health communication. Two causes, two lanes.
That changed throughout my public health journey. At MSF, I was shaped by colleagues who were already connecting these dots, including Maria Guevara, a good friend and mentor who was among the voices pushing planetary health from the margins to the center of humanitarian medicine. At WHO, I witnessed zoonotic outbreaks and extreme weather events hit the same communities, sometimes in the same season, and with the same health system unprepared and under-resourced for either.
By the time I went back to university for my Master of Public Health degree in the UK in 2023, the question I wanted to answer had already formed: what does it actually take to build a health system that can withstand a warming world? My research focused on climate-resilient health systems in the Philippines, and the roles and practices of the local health workforce in building them.
This guide is for people who know that instinctively — or are beginning to — but want a clearer map of the territory. Whether you’re a health program manager, a communicator, a clinician, or a development professional who keeps seeing climate come up in your work, this is a place to start.
This resource covers the science behind climate change, its impacts on people’s health, and what a meaningful response looks like in practice.
Understanding the science
These two terms are often used interchangeably, but they’re not quite the same thing.
Think of global warming as the core phenomenon: the planet’s average surface temperature rising over the long term, driven primarily by how we produce and use energy. Climate change is what global warming sets in motion: shifting rainfall patterns, rising sea level, more intense storms, and longer droughts. NASA draws this distinction clearly: global warming is a single measurable trend; climate change is the cascade of consequences that trend produces. One is the cause; the other is everything that follows.
🧐The #WarmingStripes chart below shows the Yearly Average Observed Temperature Anomaly, or the difference between the pre-industrial baseline from 1850–1900 and the annual global surface temperature since then. The World Meteorological Organization (WMO) confirmed that 2025 was “one of the warmest years on record” and the past decade was the warmest decade on record, as you can see in the deep red shades on the right of the chart.
Weather is what happens outside your window today: it’s the temperature, the rain, the wind. Climate is the pattern of weather over decades. A single hot day is the weather. A trend of increasingly frequent extreme heat events over several decades is climate change.
This distinction matters because people sometimes point to a cold spell as evidence against climate change. Climate science is not about individual events. It’s about long-term patterns and their consequences.
🧐 NASA explains why it’s important to keep an eye on both the weather and the changing climate.
The word anthropogenic simply means “caused by humans.” Most climate scientists agree: the primary driver of today’s climate change and global warming is “unequivocally” human activity.
Here’s the mechanism: when we burn fossil fuels, we release carbon dioxide and other greenhouse gases into the atmosphere. These gases act like a blanket around the Earth. They let sunlight in but trap heat that would otherwise escape into space. The more greenhouse gases we add, the thicker the blanket, and the warmer the planet gets. This is the greenhouse effect, and at natural levels, it keeps Earth livable. The problem is we’ve been thickening that blanket at an unprecedented rate since the Industrial Revolution.
Natural factors — volcanic eruptions, changes in solar activity, shifts in Earth’s orbit — do influence climate, but they can’t explain the rate or pattern of warming we’re seeing now. “The evidence for human influence on the climate system was found to have progressively strengthened,” stated the Intergovernmental Panel on Climate Change (IPCC). The chart below from the Climate Change Tracker differentiates natural climate variability or observed warming from anthropogenic causes or human-induced warming.
But “human activity” doesn’t mean human activity equally. Research published in Scientific Reports found that 20 of the 36 highest-emitting countries are among the least vulnerable to climate change, while 11 of 17 low-to-moderate emitters are acutely vulnerable to its impacts. Pacific Island nations contribute less than 0.03% of global greenhouse gas emissions, yet face existential threats from sea level rise and intensifying storms caused by emissions produced elsewhere. This mismatch between who caused the crisis and who bears the cost is precisely what the loss and damage framework addresses: the recognition that climate change is already causing irreversible harm to communities that did little to create it, and that the global response must include accountability and reparative support or a “just transition.”
🎧 Listen: The BBC’s The Climate Question podcast offers a clear, accessible explainer on the mechanics of climate change. Experts stress that every fraction of a degree of warming matters, meaning it’s never too late to take meaningful action. Ultimately, they encourage civic engagement and political participation as essential tools for driving the systemic changes needed to protect the planet.
These two terms come up frequently in policy discussions and refer to different but necessary strategies. The IPCC defined these terms as follows:
Mitigation means reducing the causes of climate change, for example, cutting greenhouse gas emissions, transitioning to renewable energy, and reducing deforestation. It’s about preventing further warming.
Climate TRACE data found that greenhouse gas emissions fell in the power sector, but rose across fossil fuel operations, transportation, manufacturing, and buildings, pushing overall emissions higher.
The healthcare sector also contributes to this, accounting for 4.2% of global greenhouse gas emissions, as reported by the 2025 Lancet Countdown on health and climate change. Some mitigation strategies include reducing emissions from health facilities, shifting to renewable energy, and implementing more sustainable alternatives for waste management and supply chain.
Adaptation means adjusting to the climate changes that are already happening or are locked in. For health systems, this might mean designing heat-action plans, preparing for more frequent flood-related disease outbreaks, or building health facilities that can withstand extreme weather. Training the health workforce to prepare for and respond to climate change, as well as supporting them to promote behaviors that deliver simultaneous benefits to people’s health and address climate change, are examples of adaptation strategies.
🔗 Read Tracking Health Impacts and Building Health System Responses below for more details on climate-health initiatives.
No. This is one of the most important things to understand, and one of the most frequently misread messages from climate science.
The science does not say, “it’s too late.” It says: the longer we wait, the more damage is locked in, and the harder and more expensive it becomes to protect people’s health and wellbeing. Every fraction of a degree of warming we prevent matters. Every year of delay has consequences, but so does every year of action.
And action is happening. The Alliance for Transformative Action on Climate and Health (ATACH), a WHO-led global platform established at COP26, has grown to over 100 countries committed at the Ministerial level to building climate-resilient, low-carbon health systems. This means health ministers from every region of the world agree that climate change is a health system problem that requires a health system response. The political foundation for climate and health now exists in a way it didn’t a decade ago.
At COP30 held in Belem, Brazil in 2025, health had a dedicated space for the first time at this scale. WHO’s Health at COP30 programme brought together health sector voices, including clinicians, researchers, policymakers, and community advocates, to ensure that climate negotiations don’t continue treating health as a footnote. This shift mattered because research shows that the health gains of climate action — cleaner air, reduced heat exposure, fewer climate-attributable deaths — are routinely left out of the cost-benefit models that shape policy. Decisions made without that full picture tend to underestimate both the urgency of acting and the benefits of doing so.
There’s also a strong case for leading with health when talking about climate, not just within health systems, but in public discourse more broadly. A major review of nearly 200 studies, commissioned by Wellcome, found that framing climate change as a health issue increases engagement across the political spectrum, including among people who aren’t already concerned about climate change. Health makes the issue immediate and personal in ways that emissions charts and temperature projections often don’t. Most of the research comes from the United States, the United Kingdom, and Canada, so how this translates across Asia Pacific contexts is still an open question, and one that practitioners in this region are well-placed to help answer.

The 2025 Lancet Countdown is clear-eyed about where momentum is coming from. Even as some governments backslide on commitments, other actors are filling the gap: local governments, civil society organizations, community-led movements, and the health sector itself. The report frames this as an “all hands on deck” moment.
Tracking health impacts
Scientists have used detection and attribution as a way to isolate climate change’s contribution to a health outcome from all the other forces at play. It’s not simple. It requires long-term data, careful modelling of what would have happened without climate change, and accounting for the social factors that shape vulnerability.
This is why tracking efforts like the Lancet Countdown on health and climate change matter. Now in its ninth year, the 2025 Lancet Countdown report — produced by 128 researchers from 71 institutions worldwide — monitors 57 indicators linking climate change to health outcomes across five domains. It is the most rigorous longitudinal effort to document what is happening to human health as the climate shifts. The 2025 findings are the starkest yet: 12 of 20 indicators tracking health risks have reached record levels. Heat exposure alone caused an estimated 640 billion lost labor hours in 2024. Droughts and heatwaves pushed an additional 124 million people into moderate or severe food insecurity in 2023.
So how exactly does climate change affect human health? Scientists describe two broad pathways.
Direct impacts are the most visible: the heat that kills, the flood that drowns, the wildfire smoke that fills lungs. These are immediate and physical. Heatwaves kill the elderly in cities with insufficient cooling systems. Typhoons destroy the health facilities that communities depend on. Floods contaminate water sources and displace families into overcrowded evacuation centers where disease spreads.
Indirect impacts are slower, more diffuse, and in many ways more insidious. Climate change reshapes the biological and social environments that determine whether people stay healthy. Warmer temperatures and shifting rainfall patterns expand the geographic range of mosquitoes that carry dengue and malaria, diseases now appearing in places and seasons where they were previously unknown or even eliminated. Rising seas and intensifying storms force displacement, affecting community structures, access to care, and social networks that buffer people’s well-being. Disrupted agriculture and fisheries drive food insecurity and malnutrition. For example, in Pacific Island countries, where local food systems are being degraded by coral bleaching, saltwater intrusion, and increasingly severe storms, communities are turning to cheap imported ultra-processed food as the only affordable alternative. This dietary shift is fuelling a double burden: climate change deepening food insecurity while simultaneously driving the noncommunicable diseases (NCD) epidemic of obesity, diabetes, and cardiovascular disease that Pacific nations are already disproportionately carrying.
The IPCC’s Sixth Assessment Report maps these pathways in detail, including how they interact with existing vulnerabilities — age, income, housing, health system access — to amplify harm for those already on the margins.
WHO summarizes climate change impacts, exposure pathways, and vulnerability factors in this diagram.
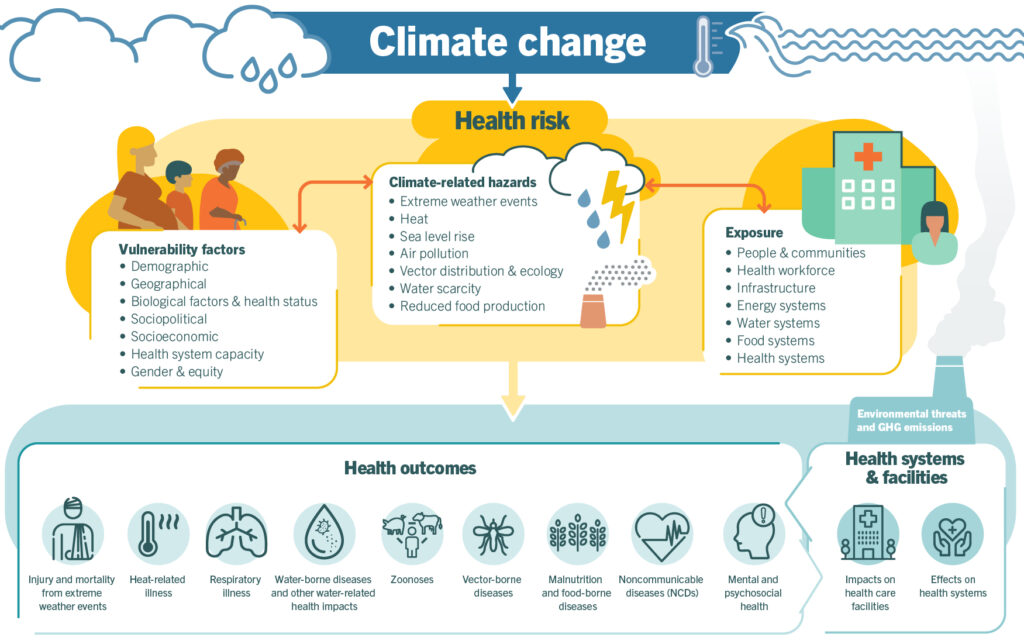
The critical point that the Lancet Countdown, IPCC, WHO, and other authorities on climate and health are making is that these pathways don’t operate in isolation. A community hit by a typhoon faces immediate injuries and contaminated water and a disrupted health system and the psychological toll of displacement — often all at once. Understanding climate and health means understanding these cascading and compounding effects.
The Asia Pacific picture is sobering. Pacific island nations face an existential version of the climate-health crisis: low-lying atolls are losing land mass to rising seas, already forcing some people to leave, and with them goes their access to health care, their community networks, and their sense of home. The 2026 Lancet Commission on Sea Level Rise underscores the particular exposure of coastal and island populations across the region to compounding climate risks.
However, the 2024 Lancet Countdown report on Small Island Developing States reveals that while many Pacific nations have formally acknowledged climate displacement in policy, very few have translated that into health vulnerability assessments to shape how resources get allocated.

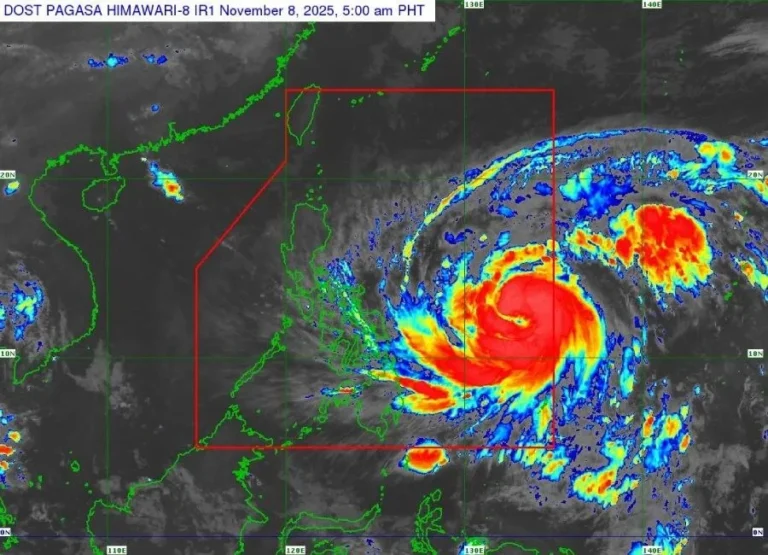
For the Philippines and Southeast Asia more broadly, the risks compound differently. Typhoon intensity is increasing. A World Weather Attribution research found that climate change made the potential intensity of typhoons in the Philippine Sea around 1.7 times more likely in 2024. The clustering of six typhoons in November 2024 was never witnessed before in the Western Pacific basin, but such an event can be more frequent in the coming years, affecting lives, livelihoods, and infrastructures.
Another trend closely monitored by epidemiologists is the shift in dengue transmission seasons, with warmer temperatures allowing Aedes mosquitoes to thrive for a longer period. A 2025 study across 21 countries found that rising temperatures were already responsible for 18% of dengue incidence in Asia and the Americas between 1995 and 2014, with cases projected to rise by up to 76% by 2050.
In addition, heat stress is making outdoor and agricultural work genuinely dangerous for the millions across Asia Pacific who have no choice but to work outside, with workers in tropical and subtropical regions carrying the highest heat burden of any sector globally.
🌏 Explore: Lancet Countdown Asia Regional Hub | ClimaHealth — Asia Pacific resources | Global Heat Health Information Network’s Heat at Work
The standard answer to “who is most at risk from climate change” tends to list demographic categories — the elderly, children, the poor — and move on. That framing is accurate but incomplete. It describes groups without naming the specific ways climate change compounds their existing vulnerabilities, or why those vulnerabilities exist in the first place. Here’s a clearer picture.
Pregnant women and newborns. The physiological changes of pregnancy alter how the body regulates heat, making pregnant women significantly more vulnerable to extreme temperatures. A 2024 meta-analysis across 66 countries found that for every 1°C rise in temperature, the odds of preterm birth increase by around 4%, and during heatwaves, the risk rises sharply. Higher temperatures have also been associated with increased rates of stillbirth, gestational diabetes, and congenital anomalies. The risks are concentrated in low- and middle-income countries, where preterm birth rates are already highest and cooling infrastructure is least available.
Agricultural and outdoor workers. People who work outside have no option but to move indoors when temperatures become dangerous. According to the ILO and GHHIN, workers in tropical and subtropical regions, where agriculture accounts for a large share of employment, face the highest heat stress burden of any sector. The agricultural sector alone accounted for 83% of all working hours lost to heat stress globally, and a chronic kidney disease epidemic of unknown origin has been documented among farmworkers in hot regions, including Southeast and South Asia, linked to repeated occupational heat exposure and dehydration. Many agricultural workers have no financial safety net to fall back on. As their income depends on how much they harvest, stopping to rest, even in dangerous heat, is not always a choice they can afford to make.

People living in informal settlements. Communities without access to adequate ventilation, cooling, or reliable clean water are structurally unable to protect themselves from heat or from the waterborne diseases that follow floods. It’s the direct health consequence of housing insecurity and under-investment in urban infrastructure.
People with pre-existing health conditions and disabilities. People living with respiratory conditions like asthma are made more vulnerable by worsening air quality from wildfire smoke and heat-intensified pollution. People on psychiatric medications are at particular risk during heatwaves. Antidepressants, antipsychotics, and related drugs can interfere with the body’s ability to regulate temperature, alter heat perception, and, in some cases, cause dehydration-related complications. Heatwaves have also been associated with a 9.7% increase in mental health-related hospital presentations.

Indigenous peoples. The climate-health burden on Indigenous communities goes beyond physical exposure, as land is a key determinant of their cultural identity, mental health, and well-being. As climate change degrades access to traditional territories through flooding, drought, and displacement, the psychological consequences include grief, anxiety, depression, and loss of cultural continuity. A systematic review found that Indigenous peoples globally are disproportionately affected by climate-related mental health harm, compounded by pre-existing social inequities and limited access to culturally appropriate care.

People deprived of liberty. Incarcerated people are almost entirely invisible in climate and health policy discussions, yet they are among the most exposed. They cannot relocate when conditions become dangerous. Many facilities lack adequate ventilation or cooling. In the Philippines, ICRC mapping found that roughly a quarter of the country’s 130,000 detainees are held in jails located in areas at high risk of floods, typhoons, heatwaves, or landslides, in facilities already running at a 314% congestion rate. When a disaster hits, evacuations are last-minute, medications and medical records are lost, and families often have no idea where their loved ones have been taken. The ICRC’s Prisoners of Climate Change programme, developed in collaboration with the Bureau of Jail Management and Penology, is working to address this, and the mapping approach is now being extended to Bangladesh, Sri Lanka, and Cambodia, where 2020 floods displaced nearly 3,000 detainees across the country’s worst-affected prisons.
On mental health more broadly, climate change affects psychological well-being through multiple pathways: direct trauma from extreme weather events, displacement and loss of community, eco-anxiety among younger generations, and cumulative stress on health workers and responders who face repeated crises. Research consistently shows that the populations above carry the heaviest mental health burden, too: those already facing poverty, marginalization, disrupted land access, and limited healthcare are also least equipped to absorb repeated psychological shocks.
The climate crisis is not a great equalizer. It is a multiplier of existing inequities, and its worst health consequences fall on people who are already underserved by the systems meant to protect them. Any response that doesn’t start from that understanding will keep missing the people who need it most.
Building health system responses
Call to Action: Your Turn
Climate change is a health crisis, and the people bearing the worst of it are not the ones who caused it. The evidence is clear and the frameworks exist. What’s needed now is sustained, credible, equity-centred advocacy that puts health at the center of the climate conversation.
Take this further
- Use the Lancet Countdown as your evidence anchor. It’s the most comprehensive annual tracking of climate and health indicators available, freely accessible, and built for advocates.
- Name the financing gap. Only 0.5% of multilateral climate funding goes to health. That number belongs in every conversation about why progress is slow.
- Apply loss and damage framing in Asia Pacific contexts. The countries facing the heaviest climate and health burden contributed least to the crisis. That’s the equity argument.
- Keep a One Health lens on pandemic preparedness and environmental health. Climate change, ecosystem disruption, and infectious disease share upstream drivers and need integrated responses.